
That pinch in the front of your shoulder… You were told it was a simple sprain. Rest it, do some band work, maybe get adjusted a few times, and you’d be back on the course in four to six weeks. That was two months ago.
You are back on the course — technically. But you’re not really back. You’re choking down on your irons to shorten the lever. You’re abbreviating your backswing to avoid that pinch at the top. You’ve quietly stopped hitting driver on anything that requires a full shoulder turn. Your playing partners at Saddle Rock Golf Club haven’t said anything, but your game is telling the story clearly enough: you’re managing the shoulder on every single swing, and you’ve started to wonder whether this is just what golf feels like for you now.
Here’s what nobody told you after that initial diagnosis: “just a sprain” is one of the most misleading phrases in sports medicine. It accurately describes the tissue involved — the AC ligaments — but it completely obscures the mechanical complexity of what it takes to fully recover one, especially for a golfer. The AC joint doesn’t just have to be pain-free. It has to withstand the rotational forces, the weight shift through impact, and the follow-through loading of a full golf swing — hundreds of times per round, across an entire season.
If your shoulder has plateaued, it’s almost never because the ligament hasn’t healed. It’s because the mechanical environment around the joint hasn’t changed enough to let it perform under those demands. And that’s a completely different problem than the one most standard rehab protocols are designed to solve.
Why AC Joint Plateaus Are So Common in Golfers
The golf swing is one of the most mechanically demanding movements the AC joint is asked to tolerate. At the top of the backswing, the trailing shoulder is loaded in external rotation and elevation simultaneously — exactly the position that places maximum stress on the AC ligaments. Through the downswing and impact, the lead shoulder absorbs the deceleration forces of the swing. In the follow-through, the trailing shoulder crosses the body in a movement that directly compresses the AC joint.
Do that 80 to 100 times in a round, often before the surrounding musculature is truly ready to support it, and you have a very efficient mechanism for keeping an AC joint chronically irritated even as the underlying ligament attempts to heal.
Most golfers plateau for one of three reasons — and understanding which one applies to you is the first step toward actually getting unstuck.
The premature loading trap. The AC joint is exceptionally sensitive to shear force — the horizontal stress that occurs when the arm moves across the body or overhead. Returning to full swings even slightly before the joint can tolerate that shear resets the inflammatory clock. The ligament never fully strengthens and heals because it’s being re-irritated faster than it can remodel. For golfers, this often looks like feeling fine at the range with a 7-iron and then waking up sore after the first full round. The tissue wasn’t ready for full swing volume at full intensity — it just felt like it was.
The passive care trap. Massage, chiropractic adjustments, and dry needling all serve important functions in AC joint recovery — but they treat the symptom rather than the cause if they aren’t paired with the specific scapular stability work that addresses why the joint keeps getting overloaded. If your treatment has been primarily hands-on without a progressive loading component targeting the serratus anterior and lower trapezius, you’ve been managing the joint rather than rebuilding it.
The stretching trap. Many golfers try to “loosen up” a sore shoulder by pulling the arm across the chest — a classic cross-body stretch that feels intuitively helpful. For the AC joint, it’s counterproductive. That movement directly compresses the acromion into the clavicle, which is the exact mechanical event the healing ligaments need to be protected from. The more aggressively you stretch the front of the shoulder, the more you’re working against the very tissue you’re trying to let recover.
The Hidden Contributors Nobody Is Treating
Here’s the part of AC joint rehab that most standard protocols miss entirely — and it’s the most common reason golfers plateau for months without understanding why.
The AC joint is not a standalone structure. It functions as part of a connected mechanical chain that runs from your feet through your hips, thoracic spine, ribcage, shoulder blade, and finally the AC joint itself. When anything in that chain isn’t doing its job, the AC joint absorbs the excess mechanical stress as the weakest link in the system. Treating the shoulder without evaluating and addressing that chain is like replacing a blown fuse without finding out why it keeps blowing.
For golfers specifically, three upstream contributors are responsible for the majority of chronic AC joint plateaus.
Thoracic spine stiffness. The golf swing generates its power through rotation — and that rotation has to come from somewhere. In an ideal swing, the thoracic spine (your mid-back) provides the majority of it. When the thoracic spine is stiff, as it commonly is in golfers who sit at a desk during the week and play on weekends, the shoulder complex is forced to compensate. The shoulder blade can’t wrap around the ribcage properly, the AC joint has to “hinge” more than it was designed to, and the swing rotation that should be coming from your mid-back is instead being demanded from a joint that is already compromised. Treating the shoulder without mobilizing the thoracic spine is one of the primary reasons golfer AC joint cases drag on.
Pec minor tightness. The pectoralis minor is a small muscle that attaches the shoulder blade to the ribcage. When it becomes tight — and in golfers who spend significant time at address with a rounded upper back, it almost always does — it pulls the shoulder blade into an anterior tilt: tipped forward and down. In that position, the acromion is driven toward the clavicle on every swing. You can do all the scapular exercises in the world, but if the pec minor is chronically shortened, it will continue to drag the shoulder blade back into the position that jams the AC joint. Dry needling the pec minor and subclavius is one of the most direct interventions for unlocking this pattern — releasing the tension that no amount of manual exercise can override until the tissue itself is addressed.
SC joint dysfunction. The clavicle is a strut. One end connects to the shoulder blade at the AC joint; the other end connects to the sternum at the sternoclavicular (SC) joint. If the SC joint isn’t moving correctly — which happens frequently after an AC joint injury as the body guards and restricts motion throughout the entire collarbone — the mechanical stress of the swing can’t be distributed across the full length of the clavicle. Instead, it concentrates entirely at the AC joint end. A comprehensive assessment from a sports chiropractor at Kinetic Sports Medicine & Rehab in Centennial, Colorado will evaluate both joints, because treating the AC joint without restoring SC joint mobility is treating half the problem.
The Missing Piece: Posterior Tilt and Why Most Shoulder Rehab Gets It Wrong
Most golfers who have done any shoulder rehab have been told to “squeeze your shoulder blades together.” Scapular retraction — pulling the blades toward the spine — is the foundation of most standard shoulder stability protocols, and it does serve a purpose.
But for AC joint recovery in golfers, it is almost never sufficient on its own. The movement pattern that is actually missing in the majority of chronic AC joint cases is posterior tilt — the ability to tip the top of the shoulder blade backward, away from the ribcage.
Here’s why this matters for your golf swing. Through the downswing and impact, your lead shoulder blade needs to posteriorly tilt to keep the AC joint in a mechanically sound position as the arm accelerates. Without that posterior tilt capacity, the AC joint becomes the primary pivot point for the entire arm during the swing — essentially acting as a hinge it was never designed to be. The result is chronic “grinding,” pinching, and irritation that persists even after the original ligament injury has biologically resolved.
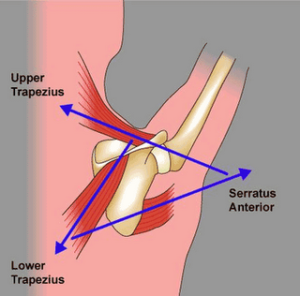
Research supports this picture clearly. Scapular dyskinesis — abnormal movement of the shoulder blade — is present in nearly 80% of chronic AC joint cases. The pain isn’t usually coming from the original tear anymore. It’s coming from the failure of the serratus anterior and lower trapezius to support the weight and movement of the arm under the demands of the sport. Until those muscles are specifically targeted and progressively loaded, the shoulder blade will continue to move incorrectly, and the AC joint will continue to absorb the consequences.
A Reassessment Checklist for Stuck Golfers
Before your next round, run through these four questions. They’ll tell you a lot about where your rehab is actually failing.
Can you breathe into your back? Place your hands on your lower ribcage and take a deep breath. If you feel your chest rise but your ribcage stays relatively still, your upper trapezius is likely hyperactive — constantly elevating and guarding the collarbone. Diaphragmatic breathing is the foundation of proper shoulder blade positioning, and it’s one of the first things to break down in chronic AC joint cases. At Kinetic Sports Medicine & Rehab, DNS (Dynamic Neuromuscular Stabilization) principles are used specifically to restore this foundation — ensuring the ribcage provides a stable platform for the shoulder blade rather than becoming part of the compensation pattern.
Does your shoulder hurt less with a narrower grip? For golfers, the equivalent question is whether choking down significantly on the club reduces the pain. If shortening the lever arm meaningfully changes your symptoms, your plateau is largely mechanical — the joint is being overloaded by the length and force of the swing, not by an unresolved structural problem. That’s actually good news: it means the tissue is capable, it just needs a smarter progressive loading approach to build the tolerance it currently lacks.
Are you still stretching the front of your shoulder? If yes, stop. Cross-body stretching and anterior shoulder stretches feel productive but actively compress the AC joint and increase instability in the healing ligaments. The front of the shoulder does not need to be more mobile. It needs to be more stable — and stretching it is moving in the opposite direction.
Can you hold a bottoms-up kettlebell at 90 degrees? Hold a light kettlebell upside down — handle in hand, weight pointing up — with your elbow bent at 90 degrees. If you can’t stabilize it for 20 to 30 seconds without significant shaking or pain, your rotator cuff is not adequately supporting the AC joint. Until that reflexive stability is present, returning to full swing volume will continue to overload the joint regardless of how the ligament feels at rest.
When Exercise Isn’t Moving the Needle: Treatment Escalation
For golfers stuck in a genuine plateau despite consistent rehabilitation effort, the clinical toolkit at Kinetic Sports Medicine & Rehab in Centennial, Colorado extends well beyond exercise prescription.
Dry needling targeting the pec minor and subclavius directly releases the anterior shoulder complex that is pulling the shoulder blade out of position and jamming the AC joint under load. For golfers, this often produces an immediate and noticeable improvement in shoulder turn range of motion — not because anything structural changed in the joint, but because the muscular guarding that was restricting motion is released.
Shockwave therapy is particularly effective for chronic Grade I and II AC joint sprains that have stalled. The AC ligaments are poorly vascularized — they receive limited blood supply under normal conditions, which slows biological healing. Shockwave therapy uses acoustic energy to stimulate blood flow and trigger collagen remodeling in exactly the tissue that has been sitting in a stalled healing state. For golfers who have been managing a nagging AC joint issue for three months or more, this is often the intervention that restarts the process.
Joint mobilization of both the AC and SC joints restores the normal glide and mechanics of the entire clavicular strut — ensuring that swing forces are distributed across the full structure rather than concentrated at the joint that’s already compromised.
For cases that remain unresolved after three to four months of comprehensive conservative care, a referral for PRP (Platelet-Rich Plasma) injection may be appropriate to biologically strengthen the ligament tissue itself. This is a last resort within the conservative care spectrum — not a first response — but it is a meaningful option for golfers who have done everything correctly and still haven’t achieved full return to sport.
What Recovery Actually Looks Like for Golfers
One more thing worth addressing directly, because it causes significant unnecessary anxiety: the visible bump.
If you have a step-off deformity — a visible ridge where the clavicle sits slightly higher than the acromion — it may not fully disappear. For many golfers, it doesn’t. And that is not a meaningful indicator of your long-term outcome. Many professional and elite amateur golfers play with visible AC joint deformities and zero functional limitation. The bump does not equal pain, and it does not equal restriction.
The metric that actually matters is not whether the shoulder looks perfectly symmetrical. It’s whether you can complete a full round — driver to putter — with full strength, full rotation, and no lingering soreness the next morning. That is the functional standard, and it is entirely achievable for the majority of golfers dealing with chronic AC joint issues when the right mechanical contributors are identified and addressed.
Ligaments do take longer to fully consolidate than muscles — a Grade II sprain can take eight to twelve weeks to feel solid under heavy loads even with perfect rehab. But “perfect rehab” is the operative phrase. Two months of passive treatment and modified swings is not the same as two months of progressive, targeted loading with the scapular mechanics, thoracic mobility, and kinetic chain deficits all accounted for. If you haven’t had the latter, you haven’t actually found out what your shoulder is capable of yet.
The Bottom Line
If your AC joint has been “healing” for months and you’re still not back to a full, unrestricted swing, the problem almost certainly isn’t the ligament. It’s the mechanical environment the ligament is sitting in — the stiff thoracic spine that’s forcing the shoulder to compensate, the tight pec minor dragging the shoulder blade out of position, the SC joint that’s absorbing none of the load, and the serratus and lower trap that aren’t doing their job on every downswing.
Those are all fixable problems. But they require a reassessment that goes well beyond the original diagnosis — one that looks at the shoulder as part of a connected system rather than an isolated joint, and builds a return-to-golf protocol around the actual demands of your swing.
The course is right there. Let’s figure out what’s actually keeping you from playing it the way you want to.
Still not back to full swing after months of shoulder treatment? The sports medicine team at Kinetic Sports Medicine & Rehab in Centennial, CO specializes in identifying the mechanical gaps that keep golfers stuck — and building the specific rehab plan that gets you back to full rotation, full distance, and full rounds without managing pain on every swing.